Sewage wastewater focal point of understanding the coronavirus pandemic
As Sweden enters its Coronavirus critical phase, sewage wastewater becomes a focal point of understanding SARS-CoV-2.
The country’s chief epidemiologist Anders Tegnell warned the Swedish public that a new intensive phase of the Coronavirus outbreak is headed their way. Testing Sweden’s wastewater for the presence of SARS-CoV-2 now plays a major part in the effort to better understand the virus’ reach among the general public.
Sewage water can reveal what testing cannot, that is, the real scale of the virus and how many people it might have actually affected.
This kind of testing could also serve as a future early sign of a second coronavirus wave, according to Swedish scientists.
Sweden’s state epidemiologist Anders Tegnell
It takes only 3 days for the novel coronavirus to appear in human faeces. This poses a major scientific discovery because in the understanding of the disease as it means that the virus can be detected much sooner; especially if people wait to display symptoms of COVID-19, which can take up to two weeks.
Monitoring wastewater could give officials a much needed head start, allowing them to take measures on time and avoid a larger outbreak.
Although this type of early warning cannot pinpoint the exact person who’s having coronavirus in their system, it can alert the authorities about the virus’ arrival in a given community and allow for an immediate lockdown of these affected areas.
As the country entered an intensive phase, the Swedish government plans to introduce tax breaks for small companies and bring stranded Swedes home.
Testing wastewater for coronavirus is not a Swedish invention. In fact, many research groups around the world began testing wastewater for SARS-CoV-2 in a bid to place a reliable estimate on the overall number of infected people in a particular community, as many of the people there would not be tested.
Until now, research groups have found such wastewater tracer in the US and the Netherlands.
Despite the widespread shut-downs
Another major obstacle for doing such research is the limited number of reagent to conduct such testes as well as the global shut-downs of laboratories and universities that could carry such an ambitious task. Research groups are already experiencing shortages due to the economic strain while governments are in a race to come up with a working vaccine to end it all.
Cetecioglu Gurol, Associate Professor at the Division of Resource Recovery organization, and whose research focuses on recovering biochemical resources from wastewater, warns that recovering the coronavirus from sewage is much more difficult than expected as wastewater is far more complicated than regular contaminated liquids, adding that “there are a lot of things in it besides the virus.”
Meanwhile in the Netherlands
The dutch authorities aim at reaching the same estimate as their Swedish counterparts, intending to test the wastewater from more than a million of people.
Such wastewater surveillance on a massive scale could account for the people who have not been tested, says microbiologist Gertjan Medema — the chief microbiologist at KWR Water Research Institute in Nieuwegein, the Netherlands.
Detecting the SARS-CoV-2 genetic material is not as easy as it may look
The goal of “diving” head first into wastewater is to prevent the coronavirus infection from spreading covertly again causing a new massive outbreak among the population.
The entire process rests on making accurate RNA extrapolations of the amount of infected people–who would remain under the radar–by determining the scale of the infection from dirty water samples.
The main challenges of doing so is making sure that the samples obtained by mass testing are truly indicative of what is excreted by the population and not just a misleading snapshot.
Wastewater surveillance hence needs to be conducted properly and be feasible in the long run.
Wastewater as the new early warning sign of COVID-19
Wastewater testing can become the new early-warning sign of a second wave, says Ana Maria de Roda Husman, an infectious disease researcher at the Dutch National Institute for Public Health and the Environment.
Before the coronavirus outbreak, the Institute has been monitoring the sewage water for the presence of novovirus, poliovirus, measles and antibiotic-resistant bacteria.
A coordinated effort between Sweden and China
The Chinese team in charge of the coronavirus force in Beijing looks on the future cooperation between China and Sweden as a mutually beneficial relationship
In 2019, the Chinese IVL kick-started its project to treat pharmaceutical residue in wastewater in a wastewater treatment plant in Sweden.
This type of cooperation would be of extreme importance in the overall effort to handle the coronavirus pandemic in both countries.
Clinical trials for a COVID-19 vaccine are under way in Oxford
The prototype vaccine named ChAdOx1 nCoV-19 has been administered to 1,112 healthy volunteers, part of a University of Oxford vaccinated group.
The clinical trial with the upcoming “Chadox” vaccine will produce definitive results about its effectiveness against the COVID-19 pandemic in 6 months time, when final assessment about its efficacy will be made.
What needs to be assessed is the ability of candidate vaccine to create an immune response strong enough to tackle the novel coronavirus.
So far Oxford University is feeling rather optimistic about its vaccine development and plans to produce millions of doses before the end of 2020.
The first phase of the clinical trial was initiated on April 23. The vaccine is based on the common cold virus, called adenovirus.
The new vaccine construct uses the adenovirus to create a material similar to the genetic code of SARS-Cov-2 in order to make a spike protein.
The spike protein plays a vital role in connecting to particular human receptors of cell surfaces and in turn help the body react to it and make antibodies against the spike protein.
This immune response will stop the virus from entering the cells in the first place and cause the COVID-19 infection.
Safe, but has some side effects
Oxford University has been using adenovirus vaccines on 320 volunteers who took it really well. The vaccine is deemed safe although it has some side effect like headache, fever and soreness in the arm.
So far the ChAdOx1 nCov-19 experimental vaccine has been tested on six macaque monkeys, managing to successfully protect them from the virus for almost a month, boosting the confidence of the Oxford researchers about its efficacy.
Until now around 1,110 volunteers from London, Southhampton, Bristol and Oxford have been administered the candidate vaccine. Aged between 18 and 55, both male and female volunteers have taken part in the trial.
Administering the vaccines to volunteers
The participants in the human trial have been randomly selected to be injected with either the candidate vaccine or a ‘control’ vaccine such as the MenACWY vaccine, which protects against meningococcal bacteria.
None of the participants in the trial will know which vaccine they have been injected with. Then the research group will gradually assess the participants’ immune system response and evaluate the results.
When will we have definitive results?
The timeline for the trial depends on the results of phase 1 testing. After phase 1 there will be phase 2 and phase 3 trials, which may combine into one and shorten the overall trail timeline and produce definitive results sooner than expected.
If the results are encouraging enough, mass production of the vaccine will take place by the end of June and be available to the general public as soon as the end of 2020, with more than 60 million doses expected to be manufactured initially.
Boris Johnson returns to Downing Street to lead Coronavirus response
British Prime Minister Boris Johnson is back to Downing Street to take charge of the response to the coronavirus outbreak.
Mr Johnson is to chair the regular morning cabinet meeting on the Coronavirus pandemic and later talk to government officials and ministers.
The Prime minister entered No 10 on Sunday evening after Tory MPs began pressuring him to lift the lockdown.
Is this the time to ease up?
Health Minister Edward Argar announced that, accordding to him, “now is not the time to ease up” despite the growing discontent voiced from the British public.
According to the latest date, the official figures of Coronavirus deaths in UK hospitals is 20,732.
Is Boris Johnson fully recovered?
One month after Mr Johnson was told he had COVID-19 and a week in St Thomas’ Hospital, the Prime Minister is back to Downing Street to resume his full-time duties and meet with senior ministers.
It is still uncertain whether Mr Johnson will lead the press briefing scheduled for Monday, but would be undoubtedly impressive to see him do so after recovering from COVID-19 and spending three days in intensive care.
Last night, on the advice of my doctor, I went into hospital for some routine tests as I’m still experiencing coronavirus symptoms. I’m in good spirits and keeping in touch with my team, as we work together to fight this virus and keep everyone safe.
— Boris Johnson #StayHomeSaveLives (@BorisJohnson) April 6, 2020
In other news:
Elon Musk says he sent ventilators to California hospitals, they say they got CPAP and BiPAP machines instead
“We received six CPAPs and we are very grateful for the gift,” said a spokesperson for Sonoma Valley Hospital. Another Californian hospital Mammoth Hospital also said it received 10 bilevel machines from Tesla. “They’re not full ventilators but there are lots of people that need breathing assistance,” a spokesperson said, calling the donation “very gracious.”
Los Angeles County officials said they received from Tesla 100 bilevel units manufactured by ResMed in late March. The Resmed devices have been donated to US hospitals and are being used as intended. These units are used for breathing and airway support, reducing the need for certain patients to be placed on mechanical ventilation.
To ease or not to ease?
Whether to ease to lockdown or to extend it is a question the public expects answered without further delay, most likely in the next few days.
Limits on daily life were enforced on 23 March, with the public asked to stay at home, businesses asked to temporarily shut down and people asked to avoid gatherings of more than 2 at time.
Currently, all ministers are obligated by law to make assessments on whether the strict rules are having the desired effect every three weeks. Next Thursday (7 May) the next evaluation will take place.
Social distancing across the UK
The current social distancing measures have caused the frustration of a large number of UK citizens, many of whom are wondering when the lockdown will end. Supermarkets have remained open as long as social distancing inside are followed.
Avoiding the second wave is top priority
China has already expecting a second wave of the pandemic as Beijing takes steps to stop a recurrence of the first COVID-19 wave. The most important decision of Mr Johnson and his team is how and when to gradually remove the lockdown announced on 23 March.
The ease off of restrictions needs to happen due to the severe economic harm and the massive strain on the NHS to handle the outbreak.
Many fear that a second COVID-19 wave would be far more deadly than the first one which makes the decision when and how to lift the lockdown a crucial point in the current situation.
Frances O’Grady, head of the umbrella group for unions the Trades Union Congress (TUC), expressed his opinion that social distancing must continue even when the lockdown is no more. Mr O’Grady also said that risk assessments in every workplace and safe transport should also remain present whether or not lockdown continues or nor.
Foreign Secretary Dominic Raab said on Sunday that social distancing would remain for “some time” in the UK and that restoring the normal way of life cannot be prolonged for too long.
What happens around the world?
Meanwhile, countries like Belgium, Germany and Denmark have expressed their intention of partially re-opening some businesses and schools.
Professor Stephen Powis, the NHS England medical director, shared during the daily No 10 briefing that: “My fear is that those curves won’t continue to be on a downward trend, but will start to go on an upward trend. We are not at a point where any of us can be absolutely confident that that’s not going to be the case.”
Meanwhile, Mr Raab insisted the government continue to fulfil is daily target of coronavirus 100,000 tests.
The end of lockdown will be decided by tests
Priti Patel has said that removing the coronavirus restrictions across the country will not be a binary choice and that the government would not give a date for the end of lockdown. The home secretary added that five tests will have to be met before schools can reopen but said giving a date ‘would be irresponsible and get hopes up’
Direct Relief is giving away $2 million for Inogen oxygen concentrators for coronavirus response
Financial assistance of $ 2 million was committed by the American humanitarian organization Direct Relief for the purchase of oxygen concentrators Inogen. In addition to the financial help for oxygen concentrators to treat patients with the new coronavirus, the organization has also ordered protective equipment and masks against COVID 19 in the United States.
Funds are being allocated to improve inventories and critical care equipment in an effort to emergency financial support for non-governmental health care facilities and to support public health efforts by state and local public health agencies.
Mobile oxygen concentrators to fight the coronavirus in China
In a response to the critical situation with the coronavirus in China and requests from Chinese hospitals treating tens of thousands of patients with Covid-19, 500 portable oxygen concentrators are to be sent to the country to help patients who may need it during recovery from Covid-19.
On February 25, senior U.S. government officials warned that Covid-19 was likely to spread to the United States. And they were right. On February 26 the first case of coronavirus transmission from a person to person after return from travel was reported in the US.
As frontline health workers are the most exposed to the new coronavirus, protecting them is a major public health priority and a major focus of financial aid. Medical staff accounts for 3.8% of confirmed cases in China and 14.8% of cases classified as severe or critical. While the overall coronavirus fatality rate has been reported to be 2.3%, it is 14.8% among patients aged 80 years and older.
The good news for US health services is that the vast majority of infections are considered to be mild so far. “Probably over 80 percent are mild,” reports Dr. Deborah Fuller, professor of microbiology at the University of the Washington School of Medicine. .
Every year, we are exposed to a number of respiratory viruses and other coronaviruses. There are at least six other types of coronaviruses that have been in the population since the 1960s. They cause a common cold, and we go through them every year. We also go through flu epidemics every year.
Flu viruses mostly affect the elderly and people with weak immune system. These two groups are usually more susceptible to respiratory diseases and common colds. So the coronavirus case is no different from what we have seen with previous flu viruses.
How to know if you are infected with Covid-19 and not just common flu?
The symptoms of COVID-19 are the same as ordinary flu. To know for certain that it is the new coronavirus, a test for COVID-19 must be performed.
If suspect that your symptoms are resembling the symptoms of the new coronavirus desease, you should call your doctor!
What are the main symptoms of the new coronavirus (COVID-19)?
If you notice …
Respiratory symptoms
Fever
Cough
Shortness of breath and breathing difficulties
Muscle ache and pain
… these could be symptoms of something more serious than the common cold.
Flu, cold or coronavirus?
Before jumping in your car and going to see your doctor with a coronavirus scare, make sure you have the flu symptoms, and symptoms of a common colds. Hospitals are cluttered with potentially infectious patients and are a great place to catch a virus if you haven’t already.
IMPORTANT: If you are experiencing flu or coronavirus symptoms, or have been in contact with a person who has traveled to a COVID-19 outbreak area, be sure to tell your doctor as soon as possible.
If you are considering packing your CPAP for a trip to the great outdoors, do not be discouraged – it can be done.
Although it may seem like a difficult task, camping with a CPAP is really not that challenging.
Sure, your tent is not the comfy bed you have at home, and, sure, there are no naturally occurring sockets out there in the wild.
But that doesn’t mean that you’ll be left stranded with your sleep apnea out there.
On the contrary, there is a convenient solution for treating obstructive sleep apnea in the wild. In fact, there are several.
Camping with CPAP is all about the right planning
To be properly prepared for camping on CPAP therapy, follow these easy pre-trip steps:
Step 1: Pack your CPAP / BPAP machine. If it is a travel CPAP and it came with a carry bag, use it accordingly for the purpose. Travel CPAPs are light and compact, so they won’t add that much of extra weight to your camping gear.
Step 2: Pack you CPAP supplies. Pack your CPAP mask (with all necessary headgear, with all the hoses and tubing.
Step 3: Power up your CPAP. Be sure to charge your CPAP’s batterires (travel models) and pack a spare battery if you have one. You don’t want your sleep apnea savior to run out of power in the middle of the night. Calculate how long each battery is going to last while powering your CPAP.
What if you don’t have extra batteries for your CPAP camping trip
The vast majority of CPAP brands offer portable DC power adapters capable of charging your device directly from the cigarette lighter.
Portable battery kits
If you haven’t extra batteries for your CPAP device, a practical solution is to use a portable battery kit that can charge a CPAP battery directly from your car.
Use a 12-volt car battery to charge your CPAP. In order to do so you’ll need a compatible CPAP 12 Volt DC battery cable adapter.
The complete camping solution: Resmed Airmini
The Resmed Airmini is the world’s smallest CPAP machine — so small it actually fits in the palm of your hand! And, the Airmini portable CPAP weighsin at only 10.6 ounces. Small, light and yet as powerful as a full blown CPAP.
It is deliberately designed as a solution for traveling while on sleep apnea therapy – be it camping, plane travel or an epic road trip across the country. The Airmini will be there beside you.
The Airmini may look tiny, but make no mistake – it packs a powerful punch when it comes to efficiency. In fact, this travel CPAP provides the same features as the best-selling ResMed AirSense 10 Auto CPAP, including auto ramp, SmartStart, Bluetooth connectivity, and advanced expiratory pressure relief.
And, it comes with Resmed’s innovative waterless humidification system, which is another great plus when going camping with a CPAP device.
Transcend Auto Travel CPAP
Another great and more affordable option for camping with sleep apnea is the Transcend Auto Travel CPAP device. Just like the Resmed Airmini, the Transcend Auto is small, light and quiet, making it the perfect companion to take when travelling.
In fact, the Transcend Auto is a pioneer in the travel CPAP category when it comes to overall efficiency and affordability.
The Transcend Auto CPAP is a compact and ultra light portable machine designed for travel enthusiasts and patients leading an active lifestyle. This widely popular automatic CPAP device comes with the Transcend’s air bearing blower technology (EZEX) for quiet and vibration free operation.
If you’re looking for big features packed in a stunningly small package, then look no further than this premium mini device from Transcend.
Sleep apnea shouldn’t be keeping you from camping!
Spending time outdoors does not mean that you have to leave your comfort zone or make compromises when it comes to your CPAP therapy.
In fact, obstructive sleep apnea should nit disuade you from camping with your family or sleeping under the stars.
CPAP Europa’s line of portable sleep apnea equipment will make it possible to go camping, while maintaining the same therapy effectiveness that you enjoy using your home CPAP.
A travel CPAP device like the Resmed Airmini is specifically engineered to take care of that.
What if you stop your sleep apnea therapy for several days?
While it may sound like a good idea to just head out in the wild camping without taking any CPAP equipment with you, it is actually a terrible idea.
Pausing your therapy comes with many negative physical and mental effects as OSA’s debilitating symptoms will reoccur almost immediately.
Why risk backpedaling on your effective treatment and experiencing OSA’s symtpoms on your trip when the solution for camping with a CPAP is right here?
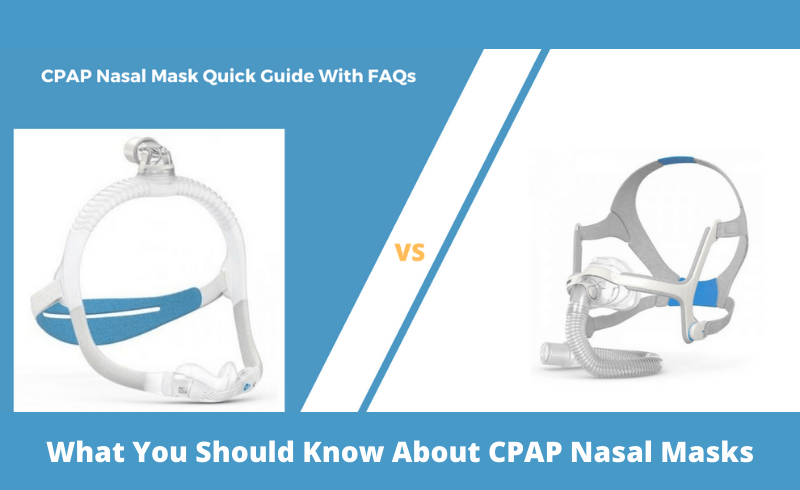
Nasal CPAP masks are one of the best options for effective sleep apnea therapy. The benefits of using a nasal model instead of a full-face masks are numerous, but, unfortunately, not many patients are educated on the subject. Nasal masks are specially suited to fit your individual therapy needs, especially if you:
breath through your mouth at night;
are a side sleeper;
feel claustrophobic wearing a full-face mask;
or just want to read / watch TV at bed before going to sleep.
Is a nasal CPAP mask better?
So why is it better to opt for a nasal CPAP mask instead of a standard full face CPAP mask? First, let’s look into what nasal and nasal pillows CPAP masks have to offer compared to full face models.
What are the advantages of nasal CPAP masks?
Nasal masks are designed to provide freedom of movement during sleep apnea therapy. They are perfect for both side and back sleepers. Therapy wise, studies have shown that nasal CPAP masks help patients achieve better adherence to their prescribed therapy, without discontinuing it.
The new-generation nasal masks are designed to offer unmatched levels of performance, comfort and thorough seal over older models.
If your CPAP setting is 10 cmh20 and higher, then a nasal masks would likely be highly recommended by your doctor. However, please note that nasal CPAP masks are NOT recommended for mouth breathers or patients whose nasal passages are blocked.
NOSE BREATHING
A nasal mask is a specifically preferred choice of CPAP users who sleep with their mouth closed and can exhale through their nose. It is comfortable to wear, unobtrusive and easy to put on and off, while simultaneously providing a steady stream of pressurized air to the sleeper’s airways.
SIZE
The smaller size of nasal CPAP masks is often preferred over full face masks. Patients who find nasal pillows uncomfortable at higher pressures opt for nasal masks instead to achieve a more comfortable and effective therapy.
What are the main advantages of nasal masks compared to full-face masks:
patients feel significantly more free in bed;
patients can turn in bed freely without risking seal bending or creaking;
patients enjoy better intimacy with their partners due to lower mask profile and less parts;
patient don’t feel trapped when we wearing a nasal mask;
patients increase their rate of adherence to their prescribed therapy.
Nasal CPAP masks come in different shapes and sizes, so most people can find a mask that works for them.
Nasal masks are less bulky than full face masks, making them less claustrophobic. Nervertheless, some patients might not get used to the contact the mask makes with the bridge nose and the upper lip.
Nasal masks support higher pressure settings without causing discomfort. And they are offered in a variety of designs including For Him and For Her.
What is the difference between nasal masks and full face masks?
The main difference between nasal masks and full face masks is that nasal masks are put over the nose instead of on both the nose and the mouth. They are connected to the patient in the same way as full face masks; that is, through a tube connecting to the CPAP machine. The CPAP / BiPAP machine then in turn, pumps the pressurized air into the patient’s airways directly through the nasal opening of the mask.
NOTE: Nasal masks cover the patient’s nose and upper lip only.
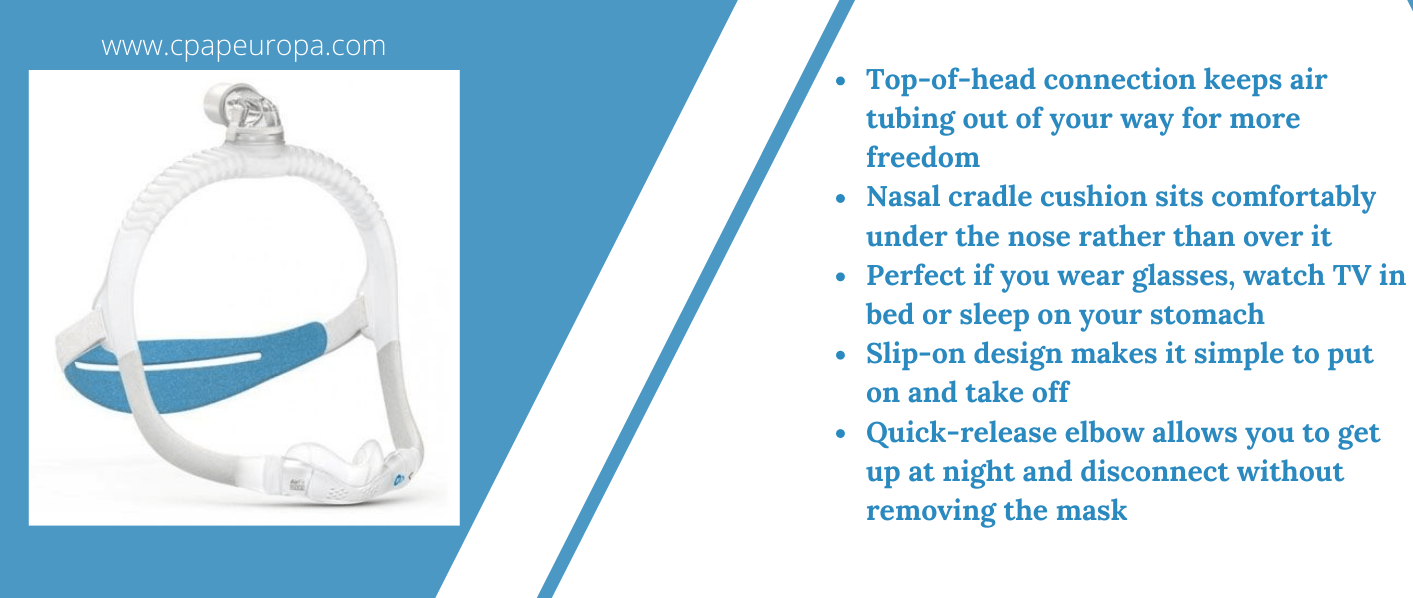
The new generation nasal masks
The latest Resmed nasal mask come with many neat features worth stating. There are even models with over the head connection, such as the ResMed AirFit N30i . The N30i is an innovative nasal mask with huge advantages over standard models.
The AirFit N30i is revolutionary mask, providing significantly less pressure on the nose and the ability to toss and turn in bed.
Less facial marks and increased mobility
The use of the nasal masks significantly reduces the number of patient complaints reporting nasal irritation and limited mobility when using full face masks. In the case of the N30i, the revolutionary design creates a “complete solution” mask focused on adherence to the prescribed therapy. This mask is specifically composed of a minimal number of parts, and is comfortable and easy to use by patients.
Resmed N30i main advantages:
Less facial marks,
Increased line of sight
Easy to put on and off;
Affordable to maintain due to less parts
Fits snugly against the face;
One of the quietest nasal masks on the market;
Successful treatment of sleep apnea requires adherence to therapy
Although effective, adherence to the sometimes life-saving CPAP therapy in most cases remains problematic. Especially for some patients who may not be accustomed to nasal masks. You can read about the severity of sleep apnea and its health effects here).
Useful tips for successful CPAP therapy
Always remind yourself that you are undergoing home sleep apnea treatment to protect your health and prevent the serious health risks untreated sleep apnea goes hand in hand with.
Talk to your partner and encourage them to share their thoughts and possible concerns about your therapy. Learn about the many benefits of CPAP therapy. In most cases, it is a therapy that saves lives. And, please, talk to your doctor doctor if you have difficulty using your mask.
Why some patients fail to adhere to CPAP therapy?
Many patients–requiring CPAP therapy to lead a normal life without the debilitating symptoms–fail to adhere to their therapy program and discontinue treatment prematurely. The reasons for this are various. Some patient for example feel somewhat uncomfortable with a large, full face mask. They can’t get used to it easily and give up. And the apnea appears again and again.
What are the disadvantages of sleeping with a nasal CPAP mask?
Although being the most preferred option for a mask, nasal models do have their drawbacks. Here are the main disadvantages of using a nasal sleep apnea mask:
They are not the most appropriate type of mask for patients who breathe mouth during sleep;
It is not recommended for patients suffering from sinusitis or a chronic condition that causes nasal congestion.
Choose a full face mask if:
You breathe through your mouth while you sleep;
Your therapy requires higher air pressure;
You have allergies or other conditions that prevent you from breathing through your nose;
You sleep on your back.
How to choose the right nasal mask?
Follow these golden rules before purchasing a nasal mask
Know your size and pick accordingly;
Choose a mask that is suitable for favorite sleep position;
Choose a masks that is easy to maintain (there are easy to find replacement parts for it.
Driving with Obstructive Sleep Apnea in the UK: Everything You Need to Know
If you live in the UK, you must tell the DVLA if you have obstructive sleep apnea syndrome or obstructive sleep apnea that affects your ability to drive safely. If you don’t, you can be fined up to £1,000 or, even worse, prosecuted if you cause an accident because of your condition. So be sure to consult with your physician if you’re not sure whether your OSA can affect your driving or not.
You and nobody else is responsible for deciding if you’re fit to drive or not. You might have sleep apnea or suffer from insomnia, or have a newborn that doesn’t stop crying at night. The reason is irrelevant. If you feel tired or sleepy during the day, to the point where it might affect your driving, then you MUST not drive. If you are told not to drive — by your GP, sleep doctor, or other medical professional — then you definitely must not drive.
Should you drive if you have Obstructive sleep apnea?
If you know that you are suffering from any form of Sleep Apnea (obstructive, central or mixed) and if you go on driving, then you are breaking the law and risking your life and the life of others around you.
If you start noticing that you are feeling sleepy during the day, do not hesitate and consult your GP. If possible, bring to them your Epworth score (Epworth Sleepiness Scale or ESS). Your GP will refer you to sleep clinic where further diagnostic will be performed to understand the origin of your daytime sleepiness and whether it is caused by OSA or not.
Even if it is caused by some form of apnea, it might not mean that you are unfit to drive. If your daytime sleepiness is not excessive, than you can continue to drive and the DVLA does not need to be notified.
Do you have to inform the DVLA?
If you are diagnosed with moderate or severe sleep apnea, you really must not drive and inform the DVLA. You must not drive until your sleep doctor confirms that the prescribed therapy is working and minimizing the effects of OSA on your body. In most cases you will be prescribed the most effective sleep apnea treatment option, that is, CPAP therapy (see the new AirSense 11 – UK version CPAP Device).
How to notify the DVLA?
The best way to notify the DVLA about having a medical condition that interferes with your driving is in writing instead of by telephone or e-mail.
What is excessive sleepiness and how it relates to driving?
As defined by the DVLA, the term “excessive sleepiness” should be interpreted as:
Excessive sleepiness likely to have an adverse effect on driving.
The term “drowsiness” should be interpreted also as excessive sleepiness.
Car and Motorcycle Drivers
1) If you are diagnosed with mild, moderate or severe OSA, without excessive sleepiness:
You may continue to drive as normal
You are not required to notify the DVLA.
2) If you are diagnosed with mild OSA with excessive sleepiness:
You must not drive until your excessive sleepiness is under control.
If your excessive sleepiness cannot be controlled within 3 months you must notify the DVLA.
3) If you have moderate or severe OSA with excessive sleepiness:
You must not drive until your sleep clinic has confirmed that:- Your OSA is under control;
– Your sleepiness is no longer excessive;
– You are complying with CPAP treatment.
You must notify the DVLA and send them your medical information proving that your symptoms are under control.
If your driving license has already been revoked, you can apply for it to be restored.
You must not drive until OSA has been diagnosed and the Sleep Clinic that diagnosed you has confirmed that your excessive sleepiness is being satisfactorily put under control by your prescribed treatment.
If you have mild OSA, you only need to notify the DVLA if your excessive sleepiness cannot be controlled within 3 months after beginning of treatment.
Bus and lorry (and taxi) drivers
If you have been diagnosed with mild, moderate or severe OSA but you don’t experience excessive sleepiness:
You may continue to drive. You do not need to notify the DVLA.
If you have been diagnosed with mild OSA and are experiencing excessive sleepiness:
You must not drive. At least not until your excessive sleepiness symptom has been successfully controlled.
If, within the span of three months, your excessive sleepiness symptom cannot be controlled you must notify the DVLA.
If you have been diagnosed with moderate or severe OSA and are experiencing excessive sleepiness:
You must not drive until your sleep clinic has confirmed to you that your OSA is under control, your sleepiness is no longer excessive, and you are complying with CPAP theraoy;
You must notify the DVLA. The DVLA will ask for medical confirmation that will prove that your symptoms are controlled. If your driving license has already been revoked, you can apply for a renewal.
If you are experiencing excessive sleepiness and OSA is suspected:
You must not drive until your condition has been diagnosed and the Sleep Clinic that diagnosed you has confirmed that your excessive sleepiness is being satisfactorily controlled by prescribed treatment.
If you have been diagnosed with mild OSA, you only need to notify the DVLA if your excessive sleepiness cannot be controlled within three months.
If you are noticing that you are experiencing excessive sleepiness on a daily basis, do not drive!
Seek an appointment with your GP;
Ask your doctor to refer you to a Sleep Clinic;
Download and complete the Epworth Sleepiness Scale Score Form to understand how severe your sleepiness is;
Bring the results to the Sleep Clinic and get diagnoses for Obstructive Sleep Apnea.
If you are diagnosed with Sleep Apnea, the Sleep Clinic that diagnoses you needs to provide a clear and precise answer if you need to inform in written form the DVLA or not.
You might be wondering how to stay sleep-debt free, how to avoid sleep deprivation even if you are a short sleeper, how to live healthy in a century of sleep disorders, insomnia, sleep apnea, and a plethora of celebrities boasting about how they sleep 2 hours a night and feel OK. Take Martha Stewart, for example. Here’s what she has to say on sleeping:
Not many sleep experts would ever quote Martha (unless for the purpose of utterly disapproving that statement). Especially when we look at some of Martha’s other quotes taken from her ‘Health and Wellness’ section at her website:
‘Our bodies work hard for us and we need to do our best to keep them healthy, fueled, and well-rested. […] Here is how we make sure we eat right, get enough exercise, control stress, and squeeze in better sleep…because wellness should be all of our top priority.’
Martha Stewart reportedly gets about 3-4 of shuteye each night. Reportedly, so is Donald Trump, Madonna, Jay Leno and other celebrities who like to get stuff done while sleeping as little as their body allows.
Unfortunately, being ‘healthy’ and ‘well-rested’ and 4 hours of sleep do not go hand-in-hand.
The power of the ‘power nap’
Among other historical short sleepers are Nikola Tesla (2 hours a night when in an inventing phase), Thomas Jefferson (2 hours), and Benjamin Franklin (4 hours). Tesla, for example, was a practitioner of the so-called “power nap” technique where you take a 20-minute nap during the day to recharge your mind and reinvigorate your work process.
Another great Thomas (Edison) was also an advocate of the power nap technique. In fact, for him, the lack of sleep was a badge of honor, so he had no other option but to try and get some, albeit short, time of “power nap” during the day in order to combat his fatigue.
In fact, Edison was so fond of power-naps, he had a dedicated napping cot in his office, in addition to the cot he has set up in his library and laboratory.
So the moral of the story is that celebrities and geniuses need less sleep than us mortals?
Well, not exactly. Not even close to the truth, actually. Before we go further into that, let’s mention the historical sleepers who got things done only AFTER they have received their healthy dose of sleep each night.
Ernest Hemingway:
Hemingway is just the first that comes to mind. Another genius historical sleeper is Albert Einstein, who was not a big fan of sleep deprivation, either. He slept a full 10 hours a night; sometimes even more. And, there’s also Winston Churchil, who made sure to get his 8 every single day.
But when it comes to geniuses, the finest example of a chronic sleep-lover is genius-prime Leonardo DaVinci, who took 20-minute ‘power naps’ every 4 hours of being awake!
Unfortunately, there are certain limits even with the power nap and geniuses. You cannot be carrying out a power-nap program without suffering the consequences of sleep deprivation. Your brain just hand handle it; and, eventually, rather soon than later, it will ask for a time-out, to try and recover what you have been doing to your body. If your brain fails to do so, you will be exposed to a particularly harmful sleep deprivation cycle which can have serious health risks.
At the other end of spectrum are people who have no choice but to sleep less
Sleep is more often than not caused not by a voluntary decision to work more and sleep less, but by an underlying sleep disorder. Emily Bronté is an example of chronic short sleeper not by choice or by following a ‘power-nap’ routine, but because of a terrible case of insomnia. In fact, her insomnia case was so severe that the great 19th-century poet and author of the timeless classic Wuthering Heights had to circle around her dining room table to try and get sleepy.
The only undisputed portrait of Brontë, from a group portrait by her brother Branwell.
So why is sleep that important?
Sleep is—how to put it mildly—EXTREMELY important for the body. Chronic sleep loss can be extremely detrimental to our long-term health. The genes controlling our immune system simply rely on restorative sleep to maintain the body healthy. Not getting enough shuteye may affect heart health, weight and our body’s capability to deal with stress.
Sleep deprivation impairs both the body and the mind equally negatively, with the first to fall in battle being mental prowess, decision making and ability to perform daily tasks at full capacity.
So why not just reboot our entire body and with just sleeping? Sounds easy, right? Not if you suffer from a sleep disorder such as insomnia or sleep apnea.
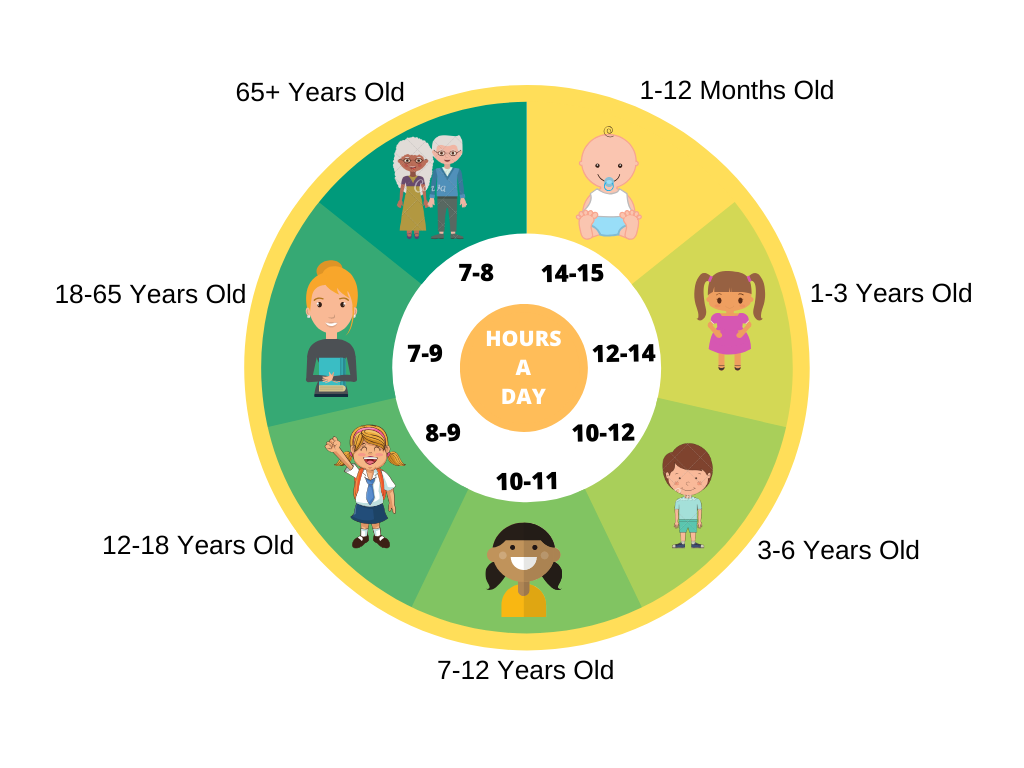
Here is how many hours of sleep you need, according to researchers and sleep experts
How is the human gene affected by sleep deprivation?
Research conducted at the Sleep Research Center at the University of Surrey, England, has shown that not getting enough restorative sleep directly affects the functionality of several hundred of genes, such as the genes responsible for the immune system, the genes controlling weight gain, cognition and heart function.
Getting enough sleep each night is vital for keeping your body and mind in healthy shape. And, when you think about it, why not—it takes so little effort to do so.
Most people work 9 to 5. In order to have enough time to prepare for work and avoid traffic, the majority of people wake early; and have no time for an afternoon nap during the day. Then the evenings come and you have to shower, prepare for dinner, read a book/watch TV, and try and get into bed as soon as possible… or else, suffer the daytime consequences.
How to improve your sleep?
Here are a few things you can do to go to bed early and have a good restorative sleep. Adopt a routine and follow it.
Leave work at work
Leave on time and also leave work behind when you go home. You can still work hard during the day, but when you enter your doorstep in the evening, make sure you leave all work-related thoughts outside. You can even leave the office later than take unfinished work home. It is really detrimental to your sleep.
Do not procrastinate your household duties and complete them on time
Once home make sure to complete your household business on time and go to bed preferably at one and the same time each night. Going to bed later than that will wreak havoc to your schedule and directly affect your sleep pattern.
Put your devices away half an hour before you go to sleep
It is of the utmost importance to not use your devices at least half and hour before you go to sleep. The short-wavelength, artificial blue light light from your TV, phone, tablet or laptop will make it harder to fall alseep because they suppress the release of melatonin. Melatonin is the sleep inducing hormone which your body naturally releases to put you at rest. If you don’t want to dusturb your circadian rhythm, make sure to go sleep.
Read in bed
Reading a book in bed both stimulates the brain and puts your entire body at ease. Reading in bed will also help with bad dreams, as long as you keep away from Stephen King’s horror masterpieces.
Do not think about work on weekends
Same as do not take work home, but applying for the weekends, too. Keep your thoughts away from how your week went at the office or what you have to do on Monday.
Healthy eating equals healthy sleeping
By decreasing the amount of saturated fats and sugar while focusing on healthier fiber-rich foods you can drift off and enter deep sleep much easier. Diet-stimulated heartburn can keep you up, so keep away from fried nor high-fat foods or alcohol. Adopt a balanced diet including fresh fruits and vegetables and low-fat proteins rich in B vitamins. It has been scientifically proven that B-vitamin foods can help the body produce the sleep-cycle regulating hormone melatonin.
Stay hydrated
Drink one glass of water just before bed. It will help you avoid experiencing thirst or dehydration while asleep. What happens during sleep is that you experience a sleep-induced fluid loss, simply by breathing. Especially if you breathe through your mouth, are a heavy snorer, or suffer from sleep apnea.
If you want to stay adequately hydrated, do not just rely on a cup of water before bed but make sure to drink non-caffeinated liquids throughout the day as well. And remember – no coffee after 6 PM.
Check yourself for sleep disorders
Did you know that there are more than 95 identifiable sleep disorders? Each with its own set of sleep-affecting symptoms. One of the most debilitating ones is obstructive sleep apnea (OSA), which is estimated to affects more than 900 million people on the planet.
To be absolutely sure that you don’t have OSA or suffer from some other form of sleep disorder, talk to your physician so they can assess your symptoms and possibly schedule a sleep apnea test. To read more about sleep disorders here.
What to do if you indeed have obstructive sleep apnea?
No one can say the exact number of OSA sufferers because the vast majority of them do not even realize they have the disorder until diagnosed. To read more about obstructive sleep apnea, please visit our Sleep Apnea guide here. To learn about the other major types of sleep disorders, keep reading.
If your sleep deprivation is caused by a diagnosed sleep disorder such as obstructive sleep apnea, you should consider starting CPAP therapy in the comfort of your home. If you have signs of sleep apnea, have already been diagnosed with OSA, or have been prescribed PAP therapy, you can purchase a CPAP machine and mask to put an end to the debilitating effect this disorder has on your sleep and health.
Losing even an hour of sleep can have a significant impact on your organism, such as your cardiovascular health, the body’s ability to fight infection, and your ability to think clearly.
The body cannot adjust easily to irregular sleep schedules (jetlag syndrome being a prime example of this). The biological clock is not a mechanical one in order to tune into a different sleep schedule by the click of a button.
Quick facts:
About 40% of adolescents and children run into a certain form of sleep problem in their development phase
Conclusion
The quantity of sleep is not as important as the quality of sleep. Even if you put 8-9 hours to bed each night, if you wake up frequently at night or suffer from a sleep disorder, chances are these 9 hours would not even matter in feeling fully rested in the morning.
Sleeping more during weekends will not make up for the lack of restorative sleep during the week. Not to mention that sleeping more during the weekend can disturb your sleep cycle and make it hard to wake up early on Monday.
The average adult needs seven hours of sleep per night, although this can lead to chronic sleep deprivation. Combined with an underlying sleep disorder, 7 hours of sleep per night is a recipe for disaster, which is why it is so important to address the problem as soon as possible. With the advancement of age, the more hours you need to get a good night’s sleep.
References
“A genetic analysis of sleep. Sleep disorder genomics and polymorphisms in circadian clock genes”. http://genesdev.cshlp.org/content/24/12/1220.full
“Lack of sleep alters human gene activity”. https://www.surrey.ac.uk/features/lack-sleep-alters-human-gene-activity
Obstructive sleep apnea is a debilitating condition causing severe pauses in breathing during sleep by partially or completely blocking the upper airways. Both partial and complete forms of apnea impact the sleeper’s oxygen intake, which in turn leads to a range of serious side symptoms and complications. There are three types of sleep apnea—obstructive, central, and mixed apnea. Today we will focus on the most widespread type—obstructive sleep apnea, or OSA. This article will discuss the risk of sleep apnea when a present genetic pattern is determined, the genetic impact on sleep apnea symptoms displayed by a subject in a risk group and how the disorder affect heart disease, hypertension and other most common side effects of OSA.
risk of sleep apnea increase the risk symptoms of sleep apnea heart disease sleep apnea include View first 3
See detailed analysis
Ask any OSA sufferer about sleep apnea symptoms and they will produce a list of these, including interrupted sleep and frequent awakenings to severe daytime sleepiness or fatigue, and, of course, the usual suspect—loud snoring interrupted by gasping sounds. Beneath the tip of the iceberg of OSA signs is an underlying bulk of health complications that the sleeper might not even suspect they are exposed to.
Among these health complications are low blood oxygen levels (hypoxemia), high blood pressure (hypertension), insulinresistance, Alzheimer’s disease and more. The disorder leads to a higher risk of stroke and heart failure, impairs your memory and ability to focus, causes morning headaches, sexual dysfunction and depression. All of the above are caused by what may seem like a simple upper-airway blockage happening at night.
The short answer to this question is: Yes, obstructive sleep apnea is partly hereditary and may run in the family. But this is the overly simplified answer. Unfortunately, nothing about sleep apnea is simple.
OSA is a condition that may be inheritable from first degree family members. For example, children can inherit from their parents their facial features, anatomical characteristics of the upper airway muscles, high body-mass index and tongue size. The anatomy of the tongue may be passed through in family history and lead to developing OSA as the tongue affects the apneic collapse of the soft tissues in the upper-airway during sleep.
The longer answer to this important query, however, needs to be grounded on scientific examination and genetics studies providing concrete results. This is what this article will explain today—the scientific approach to examining the correlation between OSA and genetics, and how exactly that relates to the broader field of study on sleep disorders up until 2020.
Inheritance across age groups and populations
Sleep disorders are present in all age groups and populations, with a strong evidence of genetic inheritance in disorders like narcolepsy and restless leg syndrome. In the case of obstructive sleep apnea the inheritance pattern is still to be defined. And while the genetic etiology of sleep apnea remains rather unclear, sustainable progress in regard to establishing a relationship between apnea and our genes has been made in recent years, with plenty of scientific data to back that up.
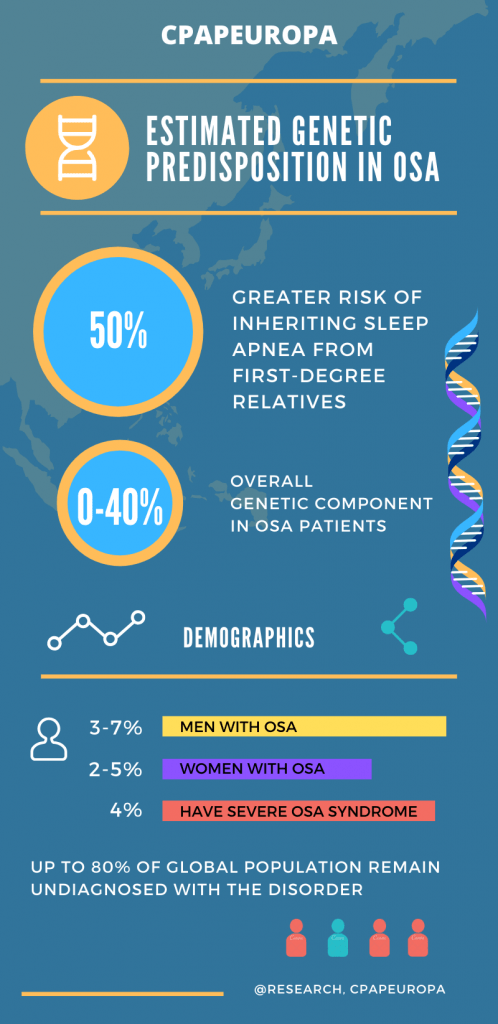
We have already exhausted the topic of risk factors in OSA cases, such as middleage, obesity and gender. The approach to establishing heterogneity and etiology in regards to OSA rests on scientific evidence acquired from documented studies with thousands of volunteering participants across all ages and gender, many of which suggest that the genetic component of OSA in the range of anything between 0 and 40%, while the rest remains in the graph secondaryfactors.
Inheritance pattern in first-degree relatives
The genetic predisposition in developing sleep apnea still remains largely undefined, in spite of the thousands of conducted studies during the last three decades. Today the inheritance patterns in obstructive sleep apnea (OSA) point to a relation between first-degree relatives with OSA and the presence of the disorder in siblings and children, where the risk of developing apnea is around 50% and greater.
As multifunctional sleep disorder OSA does have a heritable dimension researched primarily through field synopsis and genetic association examination of focus groups of participants. Conducting genetic association OSA studies aims at identifying odds ratios while exploring the connection between population-based and family-based testing. The results try to find an inheritance pattern of OSA by utilizing the existent findings in the developing field of OSA genetics through complex genotyping methods and broad genetic testing.
Genetic sleep apnea testing
Genetic sleep apnea testing analyzes alterations in chromosomes, genes, or proteins in OSA sufferers in order to confirm or exclude a genetic predisposition to the disorder. This type of testing examines the possibility that the patient developed OSA partly due to genetic passing. The methodology utilized in genetic testing is based on gene, chromosomal and biochemical gene tests.
Gene tests examine the possible variations and mutations in the lengths of DNA that could cause the disorder;
Chromosomal tests examine long lengths of DNA or chromosomes in an effort to detect major genetic alterations that could lead to the disorder;
Biochemical gene tests, examine how proteins behave and if they could change the DNA and lead to OSA.
Genetics of neck circumference and OSA explained
The relationship between neck circumference, general obesity and OSA is one of the most well-documented ones to this date. Nine in ten sleep apnea tests asks the same question: ‘Is your neck circumference greater than 17 inches (men) / 16 inches (women)’?
Obesityindex, soft palatal length and palate-to-spine angle are constantly studied through research to drive a meaningful correlation between these factors and obstructive sleep apnea. Studies have found that the link between anatomical features and OSA is not as important a factor as neck circumference.
The OSA inheritance factor in obese children
The genetic predisposition and general cause for developing obstructive sleep apnea in children relies on a variety of different factors–both anatomic and neuromuscular. Susceptibility to obstructive sleep apnea in children has proven extremely difficult and is still reliant on future studies and technological advancement. So far studies have shown that children can inherit their parent’s facial anatomy, such as large tonsils and large overbite and chin, which are factors for developing OSA.
Understanding the genetic risk factors as the first step to OSA prevention
In order to encourage early diagnosis and prevention, predictive models in genetic and phenotypic studies need to be established beyond the only suggestive framework of the current results. Steps in OSA prevention can help reduce morbidity and hesitance in the public’s approach to obstructive sleep apnea early diagnosis and treatment by educating the most genetically exposed groups of the population about the risks. The ultimate goal is to reach a proven prescriptive framework that would steer prevention and underline the benefits of early lifestyle changes reducing the chance of developing the disorder in the first place.
Why is it so difficult to understand if OSA is inherited or not?
Just like any other field of study focused on underpinning sleep disorders, genetics research of OSA is focused on early recognition and meaningful results that would increase public awareness about apnea. Until this happens, the genetic foundation of obstructive sleep apnea (OSA) still needs to be established. The difficulty in effectively studying if OSA is hereditary comes from the fact that, so far, physiological metrics across a sufficient range of genetic and phenotypic markers and participants is too costly and invasive to acquire.
The problem with the majority of genome-wide association studies trying to touch upon this extremely challenging topic is that they still remain suggestive instead of conclusive, and that most of them have not been consistently replicated.
The future of OSA genetics studies
Even with large numbers of patients taking participation in OSA studies, coverage across a wide gene region is problematic in regards to obtaining a solid statistical framework in regards to sleep apnea and its genetics origins—especially results that are robust to alternative genetic models. Genetic studies in OSA up to 2020 only find a small non-overlapping relation, without covering enough gene variants to identify a more solid ground for a positive association between the human gene and OSA. Such associations are still subject to variables posing a significant challenge to the global concern that is OSA.
Picture this. You wake up in the morning with the feeling that you didn’t sleep at all. Something was just wrong. You know you snore a lot, but snoring can’t be blamed for that, right? Well, no. But loud snoring and inability to get a good night’s sleep can definitely be a telltale sign that there is an underlying cause for both. There is a range of symptoms that can give away that there is something wrong with your sleep at night. Today we grouped them in a neat collection of top 10 sleep apnea signs that you may not be aware about. Read on to learn more about this serious sleep disorder.
More than simple snoring
You may be surprised how many people feel what we just described above. The fact is that more than a quarter of adults experience the same signs and symptoms that you may have experienced. Al lot of these are possible telltale signs of obstructive having sleep apnea (OSA).
The scary part is that you may be suffering from sleep apnea without even realizing it. If you happen to experience the following symptoms, chances are that you actually do have OSA.
If you experience one or more of these symptoms on a regular basis, schedule an appointment with your doctor to understand the underlying cause. Here are the top 10 ten sleep apnea symptoms that you should know about:
Loud snoring;
Episodic stops of breathing and awakenings during sleep;
Morning headaches;
Waking with a dry mouth;
Increased blood pressure;
Low blood oxygen levels;
Having trouble focusing;
Daytime sleepiness and fatigue;
Daytime irritability and mood swings;
Inability to get a good restorative sleep (no matter how many hours of sleep you get).
Loud snoring
Many people snore regardless of age and gender. Although not every heavy snorer has obstructive sleep apnea, the majority of OSA sufferers are also loud snorers. In fact, loud snoring is the most frequent telltale sign of sleep apnea. That is because with sleep apnea your upper airways become obstructed at night, which contributes to heavy snoring. The OSA obstruction, combined with a narrowing of the airways, creates the snoring sound that your bed partner might have become all too familiar with.
Episodic gasping for air during sleep
The meaning of the term ‘apnea’ (apnoea, Greek) means a temporary cessation of breathing during sleep. When the breathing cessation occurs, it is up to your brain to immediately understand what is happening to your body and send a panic signal to it to resume your breathing. This panic signal causes the lungs to emergency activate again, making you choke or gasp for air as your body overcomes the apnea. For as long as you experience the obstructions, these brain-stimulated micro-awakenings are going to happen. And they’ll continue to make you gasp for air again and again throughout the night–until the morning clock rings and it’s time to go out of bed and deal with the aftermath.
A combination of snoring and sleep apnea most often leads to waking with a dry mouth. And, dry mouth comes with its own group of additional complications–like sore throat, bad breath, and constant thirst. Studies have found that 1 out of three OSA sufferers that don’t use a CPAP machine experience dry mouth symptoms in the morning. On the other end of the spectrum, the majority of CPAP users stop experiencing early morning dry mouth due to their PAP devices do not even allowing the OSA obstruction to happen in the first place. What’s more, many of the contemporary CPAP devices have built-in humidifiers that prevent dry mouth.
Trouble concentrating
Starving the brain out of oxygen during apneic events inevitably affects brain function, research has shown. Studies have also shown a correlation between healthy brain chemical levels and OSA, with altered levels leading to having difficulty concentrating and memory problems.
In short, if you don’t get enough restorative sleep, your brain can’t adequately regulate the required chemicals for full cognitive functionality. This is especially true in regards to the required levels of gamma-Aminobutyric acid (GABA). GABA is the chemical responsible for staying calm and focused.
Studies have found that sleep apnea also affects the levels of glutamate, which is responsible for normal brain function.
Increased blood pressure and low blood oxygen levels
Sleep apnea causes extreme pauses in breathing during sleep. Each of these pauses causes a sudden drop in blood oxygen levels, and puts additional stress on the cardiovascular system.
During these pauses, the brain sends signals to the blood vessels to in crease the oxygen delivery to the heart so that your organism can compensate for each drop. However, the sudden increase of blood flow puts pressure on the blood vessel’s walls, which, in turn, increases the risk of high blood pressure (hypertension).
Morning headaches
Starving the brain of oxygen during apneic events causes the arteries to dilate to increase blood flow. The dilation naturally increases the exerted pressure in the head which, in combination with constantly interrupted sleeping cycle, causes morning headaches.
Daytime sleepiness and fatigue
Feeling tired all day after a ‘normal’ night with sleep apnea is one of the most common symptoms of the sleep disorder–and one of the most debilitating ones, too. In fact, any sleep-disturbing disorder comes with daytime fatigue. Your body simply cannot get the rest it needs.
Irritability and mood swings
Sure, you had a bad night of snoring and gasping for air all the time. But no one would really understand that–especially if you are constantly cranky and irritable around them. Trying to explain that your bad mood is caused by lack of a good night’s sleep and because your brain doesn’t receive much GABA chemicals is definitely an option, but hands down the best thing you can do is take action see the doctor.
Constant awakenings at night
Waking too often at night? Having to go the bathroom in the middle of your REM sleep? These are yet another ‘pleasant’ symptoms going hand in hand with sleep apnea. Irregular breathing and loud apneic snoring would most likely interrupt your sleep (and, unfortunately, your bed partner’s sleep as well).
Increased stress levels and increased risk of depression
Decreased blood oxygen levels and impaired cardiovascular system leads to extra exertion on your body, high blood pressure and high stress levels. New studies have shown that patients with obstructive sleep apnea have higher levels of the neurotransmitter glutamate and low levels of the GABA neurotransmitter. Dysfunction of glutamatergic neurotransmission is considered to be a core feature of stress-related mental illnesses.
In almost any list of top 10 sleep apnea symptoms one can run into loudsnoring, breathingpauses, soundsofchoking or gasping for air during the night, daytimefatigue and more. The point of this informational article, however, is not just to list these signs of OSA, but to convey the idea that none of these symptoms is something you should tolerate and live with. So take matters into your own hands and make an appointment with a sleep specialist who can diagnose you and recommend treatment options for sleep apnea if you indeed have one.
 deliveries for all orders over €200!
deliveries for all orders over €200!